 Hablamos Español
Hablamos Español
Treatment Options for Trigeminal Neuralgia
Medical
The use of membrane-stabilizing medications such as Lyrica or Neurontin and the elevation of the dose to adequate levels is important. These do not work like pain medicines with relief for a number of hours after a dose of the medicine, but rather, they work by maintaining a constant therapeutic blood level being reached, making regular timed dosing necessary. This level may be unique and different for each patient. It is important that the doctor increase the dose slowly to allow tolerance of the side effects and to reach a high enough level of medication to provide relief. It is common after 5-7 years for medications to stop working as effectively or at all. At this time, or earlier if the side effects interfere with functioning, then other options can be considered.
Surgery
Posterior fossa microvascular decompression is the treatment that offers the most effective long-term solution and addresses the underlying cause of the condition. This operation was conceived by Gardner but was popularized in the age of microsurgery by Dr. Peter Jannetta at the University of Pittsburgh. Dr. Stechison had the privilege of being employed on the Faculty at the University of Pittsburgh Medical Centre with Dr. Jannetta as a partner and mentor in the early 1990's. During his time there, Dr. Stechison's surgical technical experience grew as a result of the high number of these patients who came weekly from all over the world to this center where Dr. Jannetta had pioneered and contributed to the refinement of this treatment.
This surgery takes approximately 2 to 2.5 hours to perform with a 1 or 2 night hospital stay. Dr. Stechison's technique is to use a small incision behind the ear, hidden behind the hairline. A drill is used to make an opening the size of a 5 cent coin. The cerebellum is gently retracted, and the trigeminal nerve is exposed at high magnification under the operating microscope. The compressive blood vessel is identified, the vessel microsurgically displaced, and a small piece of Teflon felt is fashioned to place between the nerve and the vessel to break the point of neurovascular contact. The membrane over the brain is then meticulously sutured in a watertight fashion. The small opening in the skull is reconstructed with a small piece of acrylic, and the skin closed with some absorbable suture material under the skin.
The majority of patients (approximately 95%, typically) will awaken and not have pain, and in many cases are backed down off their medications completely. In rarer cases, the pain may not go away completely and a lower dose of medication might be required. There is a risk of recurrence of the pain of less than 10-15% over 15 years.
There is virtually no risk of facial weakness, and only a slight risk of hearing loss of approximately 1%. It is rare for there to be any sensory loss on the face unless a vein rather than an artery was the cause, and in these cases, cautery prior to division of the vein can make a micro-lesion in the surface of the nerve that can produce a very small area of numbness.
An experienced neurosurgeon who has done many of these procedures is essential as this is a delicate operation done through a very small exposure. Even elderly patients can usually tolerate this well in experienced hands as it is not a long operation.
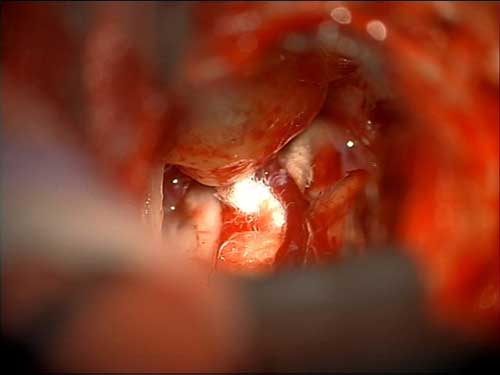
Microsurgical placement of Teflon felt between the blood vessels and the left trigeminal nerve.
Percutaneous Rhizotomy Procedures
A 4 inch needle can be passed through the face and through the base of the skull to introduce an electrode. This can be used to make a radiofrequency lesion to damage the nerve in a precise area corresponding to the pain. This approach was used commonly in the past but rarely now. Alternatively this same approach can be used to introduce a medication called Glycerol which has been used primarily in multiple sclerosis patients. Another method that can be used is balloon compression that damages the trigeminal nerve with a small inflatable balloon introduced through a needle. These methods are all associated with damage to the nerve, some sensory loss, and significant recurrence of pain.
Stereotactic Radiosurgery
This describes a radiation rather than a surgical technique. It is non-invasive with the exception of the placement of a stereotactic frame on the patient's head using some local anesthesia to introduce pins through the skin into the skull. A focused single high dose of radiation is targeted to the nerve and delivered in a single treatment. This damages the nerve and can result in relief of pain, although its onset may be delayed. The recurrence of pain following this has been debated to possibly be more difficult to treat with subsequent surgery. This is an attractive option in an elderly patient with many medical risks who might not be a candidate for a general anesthetic. One objection to the use of this treatment in an otherwise healthy patient is that it does not remove the cause, but rather damages the nerve to diminish its function in order to relieve the pain.